When the country started to reel from the effects of the new coronavirus disease (COVID-19), there was chaos because there was no handbook or established guide on how to deal with it appropriately; hence, most of us just adapted to the situation as we went along.
As we braced ourselves for the worst, we have seen the Philippine General Hospital (PGH) community weathering the storm and coming out better and stronger for it. This was only possible through the diligence, hard work and dedication of health-care workers (HCWs), as well as the outpouring of support from the general community around us in the form of donations, supplies, prayers and support.
Below are five lessons we have learned in reducing the spread of COVID-19. This is our way of giving hope to the tired front-liners, policy makers and the rest of our countrymen during this difficult pandemic.
Lesson 1: Our COVID-19 operations must be based on science, implemented with calculated precision and evaluated objectively. Nothing can be left to chance.
When the Department of Health announced that PGH was selected to be a COVID-19 Referral Center, there was very little time to convert the university hospital, but with a Crisis Command Center orchestrating the movement of manpower, equipment and processes, we were able to create, innovate and implement systems based on what was known (science), what we think we know (expertise) and what we felt was needed by our stakeholders: our patients and our staff (compassion).
An initial 130 beds were allocated for COVID-19 patients.
Then the battle against COVID-19 began: the PGH community struggled. COVID-19 was a different ballgame. Strict hospital rules particularly on infection control demanded full compliance; it felt almost oppressive with a “Do it or die” threat looming over everyone.
Eight weeks later, we paused to ask: Are we doing enough to protect our (HCWs)?
Surveillance test
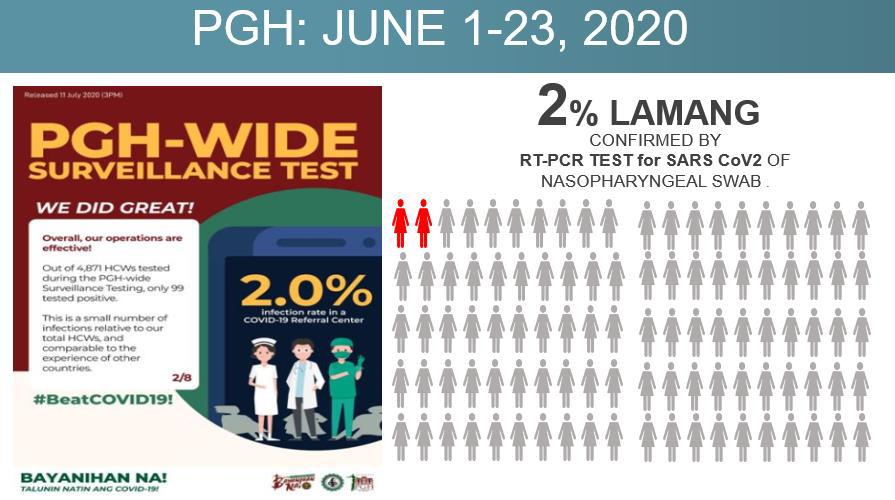
We decided to test our COVID-19 operations. We performed a hospital-wide surveillance for COVID-19 and asked PGH employees to come for COVID-19 testing using the reverse transcription polymerase chain reaction (RT-PCR) test for SARS-CoV-2 of the nasopharyngeal swab according to a schedule. These are our findings:
1) The response of our staff to the call to be tested was phenomenal. There have been many health campaigns in the history of PGH, but never did we see such all-out participation and support. A total of 4,871 from an estimated 5,000 personnel (97.42 percent) lined up to get tested. It required the organizers almost four weeks to complete testing of everyone who signed up: from June 1 to 23.
2) Key result: Of the thousands who came for testing, only 99 tested positive. While this absolute number was still high, the overall positive rate represented only 2 percent of the 4,871 tested PGH personnel. This very low infection rate is comparable to rates reported by other hospitals caring for COVID-19 patients in other countries. Even the COVID-19 Crisis Committee was pleasantly surprised.
3) But what was even more baffling is that among the 1,794 front-liners who directly handled COVID-19 patients, the ones who were the most exposed to the dreaded COVID-19 infection, working in our COVID-19 wards and intensive care units (ICUs), only 26 tested positive, or 1.4 percent.
4) Of 863 HCWs whose tasks were to support anti-COVID-19 operations, only 27 tested positive, or 3.12 percent. Support staff included those working in dietary, pharmacy, linen, security, janitorial, property and supply.
5) Of 893 HCWs who manned the non-COVID-19 wards, only 16 were positive or 1.8 percent!
6) Of 858 HCWs who were purely office-based with no direct interaction with any patient, only 10 persons tested positive, or 1.16 percent. This group included the executive offices, human resources, billing, accounting, medical records, departmental offices, engineering and IT.
7) During this time, we did not close the hospital clinic, and it continued to see HCWs who felt ill and suspected they might have symptoms of COVID-19. A total of 439 HCWs consulted the clinic during the survey period, of whom 21 were confirmed to have COVID-19, or 4.7 percent.
Point-in-time tests
8) Two services were recognized because of extraordinary zero infection rates: the Cancer Institute, with zero COVID-19 among 114 consultants, fellows and nurses tested, and the Department of Surgery, with zero COVID-19 among 130 residents and consultants tested.
We were able to establish certain “best practices” in dealing with the pandemic, among them a Crisis Command Center to orchestrate operations, a unified call center for patient queries and donations, zoning of the hospital (green, orange, red), controlled ventilation system, mandatory use of protective personal equipment (PPE) even in non-COVID-19 areas, on-site access to RT-PCR testing with 24-hour turnaround time, and more.
We will be happy to share the best practices we have learned with institutions, local governments and other health facilities.
Lesson 2: The PCR tests are only point-in-time tests. The assurance they provide is brief and lasts only up to the point one was tested. COVID-19 is so efficiently contagious that the only true guarantee that any institution is safe is when our entire community works together to get infection rates as low as possible.
But we also should have explained to our staff about PCR tests: A negative test result means that you are negative at the time you were tested. It does not guarantee you will be negative the next day, and the week after.
We were still giving each other a pat on the back when we started noticing an increase in the number of new COVID-19 infections among the staff. Weeks into the general community quarantine, our COVID-19 rates among the HCWs rapidly rose as more of our HCWs started to get infected inside and outside the hospital.

Not an island
PGH is not an island. While we know our COVID-19 crisis response system works, our hospital system is not isolated from the rest of the community. Many of our staff would go home on a daily basis and interact with family. Patients and their watchers come in and out.
Our efforts to fight COVID-19 continues to be strong and data-driven. To keep our infection rates down in PGH and in all other health facilities and workplaces, cooperation from all inside and outside PGH is needed. Our efforts need to extend beyond our hospital systems, and we must work with the community.
Lesson 3: There were two attractive ideas which we did not find helpful, and we have removed them from our routine COVID-19 operations. These are the rapid antibody tests (RATs) and the routine mass testing of HCWs. Some of the ideas that did not work for PGH have been deleted from our usual operations.
1) RATs cannot be used to screen for or to detect active infectious COVID-19. During our June hospital-wide surveillance activity, we used the donated RATs (seven different brands) whenever we had kits on the day HCWs were tested.
2) Routine mass testing of the 5,000 HCWs of PGH every two weeks is not feasible. It took us over four weeks to complete testing in the first cycle. We recognize that HCWs are at increased risk for getting COVID-19, but given the cost, operational and logistical limitations of testing HCWs every few weeks, mass testing for all HCWs is not sustainable in our institution at this time.
Instead, we recommend low-threshold targeted testing. Maintain a well-fueled, adequately staffed hospital clinic as a hub of year-round consultations and testing related to COVID-19 among HCWs. Instill initiative (“kusang-loob”) for staff to go and get tested if they start to feel sick. Simplify the testing process; the turnaround time at PGH Molecular Laboratory has gone down from five days to 24 hours. There is also a fast lane for emergency cases where the test takes only three hours for the results to be released.
Make the testing procedure also an opportunity for counseling and education. Reinforce COVID-19 information among those who are being tested, even if they are HCWs, whether by handouts or verbal reminders.
Time-sensitive
Lesson 4: Contact tracing is very important. It is also time-sensitive, thus every COVID-19 suspect and confirmed case demands that contact tracing be initiated at once.
Contact tracing loses its impact if initiated one day, one week, one month after the case is identified. Quarantine must start upon identification of a high-risk exposure. If we wait for the COVID-19 test results, as many contact tracers usually do, it might already be too late and many more persons may have already been exposed.
The window of best opportunity to intervene and make a difference is very narrow. From the time one is exposed to the time one starts being symptomatic averages four to six days in most series, and can extend up to 14 days. This is called the incubation period, the reason behind the 14-day quarantine.
To cut the transmission, persons with high risk exposure need to be identified, alerted and must voluntarily go for strict isolation.
COVID-19 patients are most infectious from one day before and up to the first three days of start of symptoms.
The only way our numbers will go down is to do immediate quarantine, as soon as exposed, and immediate testing and isolation once with symptoms. Living in the same household as a COVID-19-positive case is high risk exposure. All household contacts should go on quarantine starting on the same day the positive result is released.
The general public needs to be constantly reminded, especially by their local officials.
Lesson 5: The most valuable resource in the COVID-19 crisis is our HCWs. We must listen to what they are really saying, what they are not saying and what they are trying to say.
The crisis command team recognizes PGH HCWs and is grateful for their resilience and cooperation. The many stories of heroism and kindness as well as expressions of despair, fatigue and frustration aired on all platforms are heard and extensively discussed in weekly meetings to form the basis for constant improvements.
‘Akala ko normal’

Some issues have persisted through the months. Here are the continuing efforts of PGH to make it better for their HCWs:
• Knowledge factors: Staff cannot say “Akala ko normal lang ang may lagnat at nanginginig,” “Uminom na ako ng Biogesic kaya hindi na ako nakakahawa,” or “Kailangan ko pong pumasok dahil wala nang ibang pwedeng gumawa ng ginagawa ko.”
Not all HCWs would have the same level of COVID-19-related knowledge.
As of July 31, over 700 creative information, education and communication (IEC) materials under the “Bayanihan Na!” have been produced by our IEC COVID-19 Committee.
• Access factors: HCWs are innately “passionate” and committed and their seeming difficulty to comply to or fully support a new or changing process may be due to their inability to access certain needs.
• Economic factors: Difficulty in asking staff to stay home instead of coming to work when they are already sick may stem from loss of income, “no work, no pay” policies. Our HCWs’ call for fair compensation, salary adjustments and unpaid hazard pay are all justified complaints and urgent needs. Administration should reassure staff that these are already in the process of being addressed.
• Fear factors: It is not surprising that many sectors in the workplace experience various forms of fatigue to conquer the “fear in fighting an unseen enemy.” There is now the PPE fatigue, the quarantine fatigue and the caution fatigue. The “new normal” processes should address these new developing needs and find ways to best respond to them.
The COVID-19 pandemic is here to stay for a few more months. Let us gather our best practices and continue to learn from each other. We are one with the World Health Organization when it states what we need to getthrough this pandemic are science, solutions and solidarity.
Most of all, if there is one thing we learned from the hard work of the PGH community, it is that there is hope. We can do this! —CONTRIBUTED