

(Second of two parts)
A patient told me that their barangay official advised them that their 85-year-old bedridden mother, who had already suffered two strokes, is at high risk for COVID-19 and is considered a priority for vaccination. I advised my patient that the family has to weigh the pros and cons of vaccinating their mother more intently before consenting to her vaccination.
This highlights the need for a more rational government policy in identifying those who are suitable for vaccination, and prioritizing them.
The government should aim for a more realistic goal of vaccinating 70 percent of the population, who are suitable to be vaccinated. The qualifying word “suitable” should be emphasized. Aiming for 100-percent vaccination is either just rhetorical or even irrational, and unfounded scientifically.
The evidence is accumulating that the vaccine may even be potentially harmful to some people. It’s not a one-size-fits-all proposition. So, the government cannot just make a sweeping plan of vaccinating everyone.
Informed consent
It’s conceded that vaccination is the most viable option we have at the moment for the country to survive this pandemic. The government may even invoke its constitutionally mandated police power which is inherent in any sovereign state, and make it mandatory for everyone to get vaccinated, but I personally think that would be a bad idea.
Everyone should still be given the free will to decide. So, informed consent must be obtained before anyone gets a vaccination shot. No consent, no vaccination. Or else, the government could be accused of violating the human rights of a vulnerable population, constrained to decide out of fear.
We need a good communication plan that can lay the facts to the public as they are, and not give any impression that the pharma companies, international health agencies and national governments are keeping their cards close to their chest, unwilling to reveal information that may help the people make intelligent decisions for themselves and their country.
If there is a feeling of trust and everyone is convinced that there is full transparency on information that can impact the recipients of the vaccine, then there’s a great likelihood to get more to favor the vaccination.
It would indeed be a tragedy if our government is able to procure all the vaccine doses we need, but only a minority of the population would be willing to receive it.
Scoring system
To gain the public’s favor, we need a more rational method, consisting of an easy-to-understand explanation to convince them. We now realize that the vaccines are not exactly the silver bullet we imagined they would be. There may even be segments of the population who may be possibly at risk to suffer from significant side effects with the vaccine, like the frail and the elderly.
So, a scoring system can be drafted by our experts based on available scientific evidence, to determine those who are really suitable for vaccination and are likely to benefit from it, with no or little risk of harm.
The vaccination scoring system should determine all factors that could impact risk of exposure and getting infected, risk of severe disease, and the benefit that may be derived from the vaccine. These include age, occupation, means of transportation and pertinent medical history.
It also factors in conditions that may increase the risk of potential harm to the vaccine recipient such as old age and frailty, or presence of an unstable long-standing (chronic) disease.
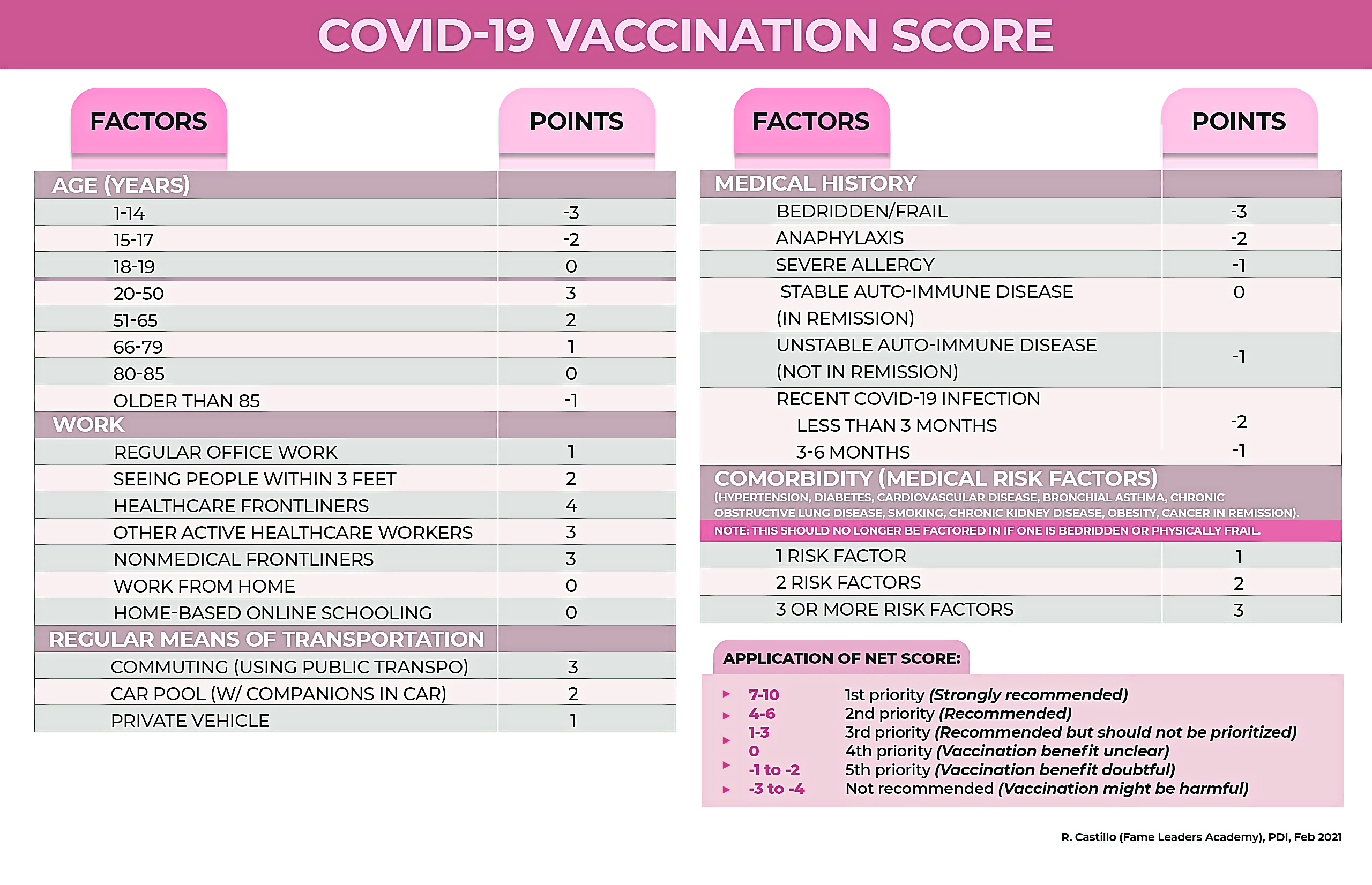
All the factors for benefits (positive points) and harm (negative points) will be given corresponding points, and the sum total of the positive and negative factors will determine their suitability for vaccination. This is illustrated in the proposed table accompanying this article.
The higher the total score, the more suitable the individual is for vaccination. Those with low scores should not be prioritized; and those with net negative scores are not considered that suitable for vaccination. The risk for harm may even exceed the potential for benefit in such patients.
In the case of our patient’s 85-year-old mother, with recurrent stroke and currently bedridden, she gets zero point for age, no score for work and means of transportation since she’s already bedridden, and a -3 points for being bedridden and frail. So her total score is -3. That makes her unsuitable for vaccination, since the potential for harm may be greater.
On the other hand, if you’re a 45-year-old traffic policeman, you get +3 for age, +3 for work as a nonmedical front-liner, +1 for means of transportation if you have your own vehicle. So, even if you have no comorbid medical condition, your total score is +7, which makes you a top priority. If you have a comorbid condition like hypertension or diabetes, your score is even higher.
A 30-year-old nurse assigned to the COVID-19 ward gets +3 for age, +4 for her work as a health-care front-liner, +3 for means of transportation if she commutes to work. So, her total score is +10 ,which really justifies her being a top priority.
Methodical and rational
With such a methodical and rational way to determine suitability or unsuitability for vaccination, it should be easier to convince suitable candidates for vaccination.
As previously explained, to achieve herd immunity, we only need to have 70 percent of the population infected or vaccinated. So that means we could afford to have 30 percent of the people unvaccinated, and this would consist of the unsuitable candidates and those unwilling to give their informed consent.
This scoring system can also serve as a guide to our implementing agencies in determining who should be prioritized for vaccination. The higher the score, the higher the priority.
If, through this scoring system, one can see there’s a clear benefit versus harm score, then one doesn’t have to mentally struggle to weigh the pros and cons.
It should also be explained that at the rate mutations of the virus is developing, there’s a big possibility that a yearly booster dose may be required. The government must already factor this in when calculating how many doses would be needed in the next two to three years. Those vaccinated this year may need another dose or two next year. The vaccine recipients will also have to set their minds that this is not a one-time, good-for-life vaccination. Just like the regular flu shots, annual booster doses most likely will be required.
But, for our personal decision-making, let’s get our shots as soon as the vaccines become available, and that is if we’re suitable using the proposed vaccination scoring. Let’s worry about the need for booster doses next year. We still have 2021 to survive.
In this pandemic, we just have to go one step at a time, but do it in a well-calculated, rational and decisive manner.