(First of two parts)
On Oct. 15, the government began the vaccination for minors against COVID-19.
We have extensively discussed the pros and cons of vaccinating adolescents and minors in previous columns (“Should we vaccinate our adolescent children?,” 6/16/21; “Should we risk the lives of 300,000 adolescents to save one?,” 6/23/21).
In the last three months, we’ve seen several previously healthy young adults less than 30 years old developing signs and symptoms of heart muscle swelling (myocarditis) which could possibly be attributed to the vaccination since there is a temporal relationship between the vaccine jab and the development of symptoms.
The usual symptoms were chest pains, palpitations and shortness of breath. They had fast heart rates with some abnormality in the heartbeat (arrhythmia).
Fortunately, their symptoms were not severe enough to require hospitalization; they improved remarkably with medications, but we don’t know how long they’ll have to take their medications, and if their hearts would revert to normal again.
Myocarditis
More than half of the cases of myocarditis would have a chronic course, meaning it may be long-standing, possibly for life. A third may have worsening symptoms, which can lead to an early death. Since we’re talking about young adults, even 20 years down the road is still too early to say farewell to this world.
We advise parents of minors to think a dozen times before subjecting their healthy children to vaccination. In the eyes of the law, minors do not have the legal capacity to make the decision for themselves, so it’s the burden of the parents to decide.
We were hoping that, due to the short supply of vaccines in the country, parents did not have to struggle with this decision yet. Hopefully, we’d have clearer data by year-end or early next year. The risk of dying from serious complications of the vaccines appear to be equal to, if not higher than, the risk of dying from COVID-19 in the near future.
The Pfizer (BioNTech) and Moderna vaccines are now allowed on adolescents aged 12 to 17. They’re both so-called mRNA vaccines, the long-term side-effects of which are still a blur. Even the one who pioneered the mRNA technology, Dr. Robert Malone, is not so confident about the long-term safety of this relatively new technology.
It’s quite apparent now that the vaccine has overreaching effects they did not initially anticipate.
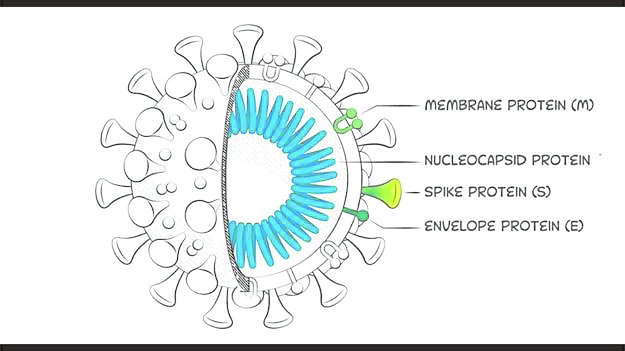
It was believed that the vaccine would only stay in the localized area of muscular tissue it was injected to, and produce just a part of the virus—the spike protein which the virus uses to latch on to the surface of its host cell, facilitating its entry. The virus has several other proteins like the membrane, nucleocapsid and envelope proteins, but vaccines like the mRNA brands only specifically produce the spike protein.
It was believed that this localized reaction would be sufficient to stimulate the immune system to produce the needed antibodies against the virus as well as the natural killer and memory cells to recognize the virus next time it’s encountered.
The vaccine-generated immunity is supposed to mount a strong immune reaction to prevent COVID-19, or if it fails to do that, at least decrease the severity of infection. So far, so good.
The body’s cells at the inoculation site produce copies of the spike protein, and the vaccine mRNA is supposed to be quickly degraded after a few days.
The mRNA was believed to be very fragile, such that it could be easily broken down by the body’s cells into harmless pieces and completely eliminated.
Real-world reactions
This mechanism of action of vaccines looked perfect in concept, but the real-world reactions apparently showed some aberrations. The experts are perplexed why, for instance, an autopsy performed by a Japanese expert on someone who died from a vaccine-related injury showed that the spike protein was abundant in all major organs of the deceased.
The vaccine no doubt was effective in generating the spike proteins, but instead of just stimulating the body’s immune system, there was an abundant production of the spike proteins, which apparently overwhelmed the body of that particular vaccine recipient.
It can be argued that it was just an anecdotal vaccine-related mishap, but even Malone, the scientist who pioneered the mRNA technology, is now saying that it’s fair to assume that the spike proteins generated by the vaccine enter the circulation and can damage any organ they lodge in.
Several other prominent virologists are now in agreement that the spike protein is not an inactive part of the virus, but actually an organ-damaging one.
Spike protein-induced injury may not be fatal but may be significant enough to cause injury to the heart, brain, liver, kidneys, ovaries and the extensive network of arteries in the body..
Since all the organs of the body have an arterial supply to survive, that means practically any organ of the body could be potentially affected by spike proteins, which could be overproduced in the body after vaccination.
Because these spike proteins are foreign to the body, the body’s immune system will try to get rid of them.
It’s this internal battle between the spike proteins and immune system cells that could be massive in some individuals, causing damage in the human body.
Since the young have apparently stronger or more robust immune systems, their reaction can be potentially more severe compared to that of the elderly.
The side effects of heart swelling with the Pfizer and Moderna vaccines are observed to be more frequent in young adults compared to seniors.
It’s a similar thing with the blood clot complication (thrombosis with thrombocytopenia syndrome) with the AstraZeneca and J&J/Janssen vaccines. It appears to be relatively more frequent in younger females below age 50.
Immunocompromised
Perhaps the pilot run of the vaccination of minors could still be justified by the guidelines that only those who are immunocompromised due to a significant comorbidity are to be included. But the guidelines must be strictly followed.
A minor who was theoretically overweight—perhaps borderline obese if you calculate his body mass index—was given the jab because obesity is supposed to be a comorbidity. But the boy is athletic and obviously healthy despite his excess poundage.
Tuberculosis is included in the list of comorbidities, but a history of primary complex (tuberculosis in children) is not enough to qualify an adolescent for vaccination. A big percentage of Filipino children are likely to have primary complex, and many recover without treatment. That even indicates they have a strong immune system.
What we’re trying to point out is that unless the minor really has a medical condition causing a weakened immune system, the parent should probably not hasten to get their children vaccinated until we have clearer data showing that the benefits really outweigh the risks.
We may have ruffled some feathers when we wrote in our previous commentaries that this recommendation to vaccinate minors is already bordering on madness. We know it’s based on experts’ advice, but it’s about time our health officials didn’t take every international agency’s recommendations hook, line and sinker, without evaluating the data themselves and making the decision based on their own appraisal of the pros and cons.
Again, we reiterate: We’re not antivaxxers. We’ve strongly advocated for targeted and protective vaccination for seniors and the vulnerable sectors of the population, but not mass, injudicious vaccination—including healthy young adults, especially minors. INQ
(To be continued)