Remember the warning in the old “Jaws” movies: “Just when you thought it was safe to go back in the water….”
We’re all excited to enjoy the outside world, and as soon as the more stringent alert levels were lifted, we wanted to make up for lost time. Kids and seniors had their field day once again in the crowded malls. This, too, became an incentive for everyone to be vaccinated, so they could have free access to the shops, some of which restricted the entrance of the unvaccinated.
In a way, it’s good. This is a healthy indicator that the public is starting to veer away from the victim’s mindset, and starting to adopt the victor’s mindset in living with COVID-19. In fact, in our columns in February and March, we proposed taking this calculated risk in opening up selected business establishments and allowing relatively low-risk individuals to go back to their work to rev up the economy. We called it a calibrated reopening of the economy, a cautious resumption of the country’s vital operations.
Generally happy
We’re generally happy with our newly revived enthusiasm in resuming day-to-day operations in our country, but we can’t help but feel some discomfort with it. We have two concerns.
First, as we tell the public to go ahead and start enjoying near-normal life once again, someone must be watching their back, so the necessary calibration could be done promptly. It must be made clear to the public which and where are the low-risk areas and activities for transmission of the virus.
We couldn’t understand why the open-air dolomite beach had to be closed down because people rushed to enjoy it. The risk of spreading the virus in such a setting is extremely low, especially if masks continue to be worn. Even if some people unknowingly have the virus, the airborne virus particles they release would get immediately blown away. The same low-risk situation can be said of parks and open-air playgrounds.
So if these areas are closed or restricted, then people would tend to go to the malls, which are more confined and where air circulation is not that good compared to open-air areas. We’ve seen media coverage of shoppers in some popular malls where reasonable distancing is an impossibility, and seniors and children seemed to have thrown caution to the wind.
Our second concern is if our experts at the Department of Health (DOH) and Inter-Agency Task Force for the Management of Emerging Infections Diseases (IATF) are closely analyzing the data and drawing some conclusions, or at least strong impressions, to guide them in any adjustment in their guidance to the public.
True, the number of new cases has plunged almost 95 percent compared to their peak levels in mid-September. True, the positivity rate has gone down to less than 5 percent in the last several days—which is the safe level indicating good control of the outbreak if maintained. But what is most disconcerting is that the percentage of people dying from COVID-19 is surprisingly increasing.
There may be an expected lag in the decrease of deaths compared to the decrease in new confirmed cases because there may be a “leftover” of the previous severe and critical cases during the surge, but this should only last a few weeks after the peak of the surge—usually two to three weeks, at most four weeks.
In our current case, it’s been eight weeks after the surge, but the number of people dying from COVID-19 has practically remained in the high hundreds, occasionally hitting 300 deaths in a singe day. In the past four weeks, our case fatality rate or the percentage of COVID-19 patients dying in relation to the new confirmed cases has more than doubled, averaging more than 3 percent, compared to the previous rate of 1.5 percent at the peak of the surge.
We hope the DOH and/or IATF could explain to the public the possible reasons for this, so they could assure all if there’s nothing to worry about, or warn if there’s something alarmingly not right in the increasing death rate in COVID cases.
Increasing death rate
Is it just an expected variance since the denominator (number of new cases) has markedly gone down? (But it’s taking too long to recalibrate!) Does it mean that the cases are now more severe or virulent? Is there a possibility that a new variant is slowly emerging that is taking advantage of the waning effectiveness of the vaccines?
The most important question that our health officials and their expert advisers must try to answer is—could this increasing death rate be an indicator of the dreaded antibody dependent enhancement (ADE)?
We raised this possible scenario in March, and recommended that our health officials be on the lookout for this potential complication of mass vaccination and emergence of more transmissible and vaccine-resistant variants. This was readily brushed off as baseless, but the emerging data seems to suggest otherwise.
I call ADE a betrayal by the body’s own antibodies. It may occur more frequently with vaccination, though it can also happen with antibodies produced from previous infection. If the vaccine can produce sterilizing antibodies and offer sterilizing immunity—that is, it can prevent transmission totally—then ADE will never happen. But if we have a so-called “leaky” vaccine with waning effectivity over time, and with a capability of the new variants to become resistant to the vaccines, then ADE may be a possibility.
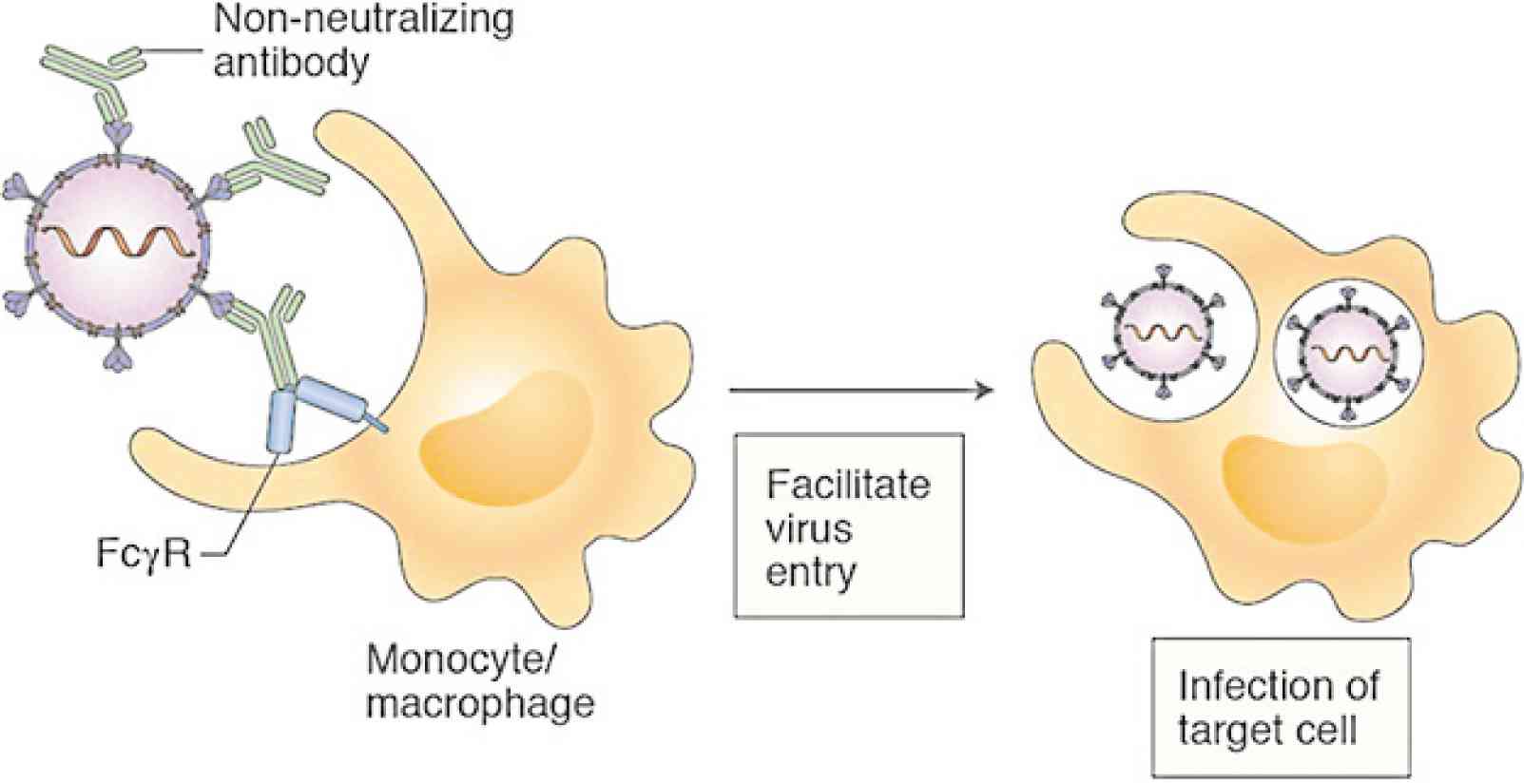
The antibodies produced by the vaccine are supposed to protect the person by repelling the virus, but since the virus has mutated already, the antibodies, which are specific to and most effective for the variant that stimulated their production, may fail to recognize these new-looking variants and even “escort” them into some immune system cells where they rapidly multiply and get released into the circulation in big quantities. Instead of being like policemen catching the bad guys (viruses), the antibodies even escort them to facilitate their entry into the cells. It’s like having police escorts to get one out of traffic.
Another explanation is that the antibodies still bind with the virus in an effort to neutralize it, but since they’re ineffective in doing so, they unwittingly facilitate the viral entry into the special cells of the immune system. These special immune system cells such as the macrophages welcome the antibody-virus complex thinking, “Hey, this guy (virus) is escorted by our policemen (antibodies), so the guy must be a good guy. Treat him well, and let him do as he pleases.” So the virus rapidly multiplies and destroys the cells.
Trojan-horse trap
Some scientists compare ADE to the Trojan horse in Greek mythology, which allowed the Greek soldiers to enter the walls of Troy and ravage the city while the Trojans were drunk and asleep because they thought the Greeks had already left in surrender, leaving behind a giant wooden horse as a goodwill gift to acknowledge their surrender.
Might we and many other countries in the world be also falling into a similar Trojan-horse trap with the COVID-19 virus? Are we celebrating too soon while the enemy lurks stealthily with another strategy at conquest?
This phenomenon of ADE is expected more in viruses coming in different subtypes or serotypes, such as the dengue virus which has four serotypes.
Infection with one serotype does not make one immune to dengue fever; in fact, it’s layman’s knowledge that the second episode of dengue fever could be worse, precisely because of ADE. It’s for the same reason inappropriate administration of the dengue vaccine to the wrong set of schoolchildren (younger than 9 years old who have likely not been exposed yet to the virus) resulted in more severe disease for some leading to death.
We hate to resurface this painful experience in our vaccination history five years ago, but it may be worth taking another look at it so as to prevent a similar catastrophe in the near future. In the case of the dengue vaccine, 800,000 children were given the vaccine and, if our memory serves us right, less than 30 died, attributed to the vaccine, but the government ordered to pull it out and stop the vaccine rollout. With the current vaccination program, we aim to vaccinate not only 800,000, not only 8 million or 38 million, but possibly a hundred million.
Are our experts taking a close look at the data of COVID-19 patients developing severe COVID and dying from it? If they involve a proportionately high percentage of vaccinated individuals already, a phenomenon that is starting to emerge in highly vaccinated countries, then it might be prudent to rule out ADE and recalibrate our mass vaccination strategy.
This is the least we could do for our people lest we be like the Hamelin pied piper in Robert Browning’s story who led unquestioning children and adults in a magical trance to their misfortune.